|
By Dr. Carolyn Dean  Signs of magnesium deficiency are everywhere in the United States, if you know what to look for. Unfortunately, the symptoms are so incredibly common that they constantly slip under the radar! Hardly anyone, especially doctors, notice that the ailments we suffer from on a daily basis are actually magnesium deficiency symptoms… and we’re all paying for it.
Just about every single person you come into contact with – especially those with a health problem, but even those with only minor complaints – are suffering in some way from this nationwide deficiency. Including you! What Exactly Is Magnesium? Magnesium is life. It is the fourth most abundant mineral in the body, right next to sulfur (which is just as important). Along with being a mineral, magnesium is also an electrolyte. “Sports drinks” (aka sugar-filled scams) claim to contain electrolytes such as magnesium, potassium, and sodium because we sweat away these important nutrients during exercise, and their deficiency is what leads to the common problems athletes face, such as muscle cramping. But believe me – electrolytes (especially magnesium) do so much more than treat and prevent muscle cramps. First off, electrolytes are what allow us to be living, electrical beings. They are responsible for all electrical activity (and thus brain conductivity) in the body. Without electrolytes like magnesium, your muscles can’t fire, your heart cannot beat, and your brain can’t receive signals. Simply put, we need magnesium to stay alive. As soon as we don’t have enough of it, we start to lose the energy and conductivity that keep us going. Technically, as soon as we become deficient, we slowly begin to die, getting more aches and pains day by day, feeling worse year after year. I can’t stress it enough… signs of magnesium deficiency are everywhere, if you just look. Magnesium is a cofactor in over three hundred reactions in the body, necessary for transmission of nerve impulses, temperature regulations, detoxification in the liver, and formation of bones and teeth. However, magnesium shows its true power in cardiovascular health. The Weston A. Price Foundation writes, “Magnesium alone can fulfill the role of many common cardiac medications: magnesium inhibits blood clots (like aspirin), thins the blood (like Coumadin), blocks calcium uptake (like calcium channel-blocking drugs such as Procardia) and relaxes blood vessels (like ACE inhibitors such as Vasotec) (Pelton, 2001).” Nearly EVERYONE has signs of magnesium deficiency, but we don’t realize it…Symptoms include:
Anything that makes you tense and tight could potentially be caused by magnesium deficiency. If you can’t relax or you can’t stop — think magnesium! Full-blown health problems can even be tied back to this crucial mineral. Most people with ANY chronic disease or issue benefit greatly from magnesium supplementation therapy. This is because chronic illness = stress, and stress depletes magnesium. The following are conditions that are likely to have magnesium deficiency as a part of the puzzle:
“Patients with diagnoses of depression, epilepsy, diabetes mellitus, tremor, Parkinsonism, arrhythmias, circulatory disturbances (stroke, cardiac infarc- tion, arteriosclerosis), hypertension, migraine, cluster head- ache, cramps, neuro-vegetative disorders, abdominal pain, os- teoporosis, asthma, stress dependent disorders, tinnitus, ataxia, confusion, preeclampsia, weakness, might also be consequences of the magnesium deficiency syndrome.” – Journal of the American College of Nutrition Amazingly, the article referenced above even mentions neuro-vegetative disorders as a possible result of magnesium deficiency. This would include comas. Stress hormone production requires high levels of magnesium and stressful experiences can immediately lead to complete depletion of magnesium stores, which might help explain why we see comas after traumatic accidents/injuries. As I mentioned above, magnesium is an electrolyte responsible for brain signals and conductivity. Without magnesium, people in comas may not be able to come to and resume conductivity. Many people with diabetes — also listed as another possible consequence of magnesium deficiency — also fall into diabetic comas. Could this be a factor in diabetic comas as well? I think further research is certainly warranted to find out. Cravings? Do you crave chocolate? Why, when people are stressed out, do they go for chocolate? Chocolate is one of the highest food sources of magnesium. Magnesium is associated with so many disorders that Dr. Carolyn Dean of the Nutritional Magnesium Association has devoted an entire book to discussing how she has treated thousands of patients for a wide array of diseases, with magnesium as the primary component. Her book, The Magnesium Miracle, is a must-read if you have any of the magnesium deficiency symptoms above, or any health problems in general, as there is likely a magnesium component to everything. Check out “50 Studies Suggest That Magnesium Deficiency Is Killing Us.” Why Don’t Doctors Find Magnesium Deficiencies In Tests?Unfortunately, conventional medicine has not woken up to the amount of research that has been done on magnesium deficiency. One of the reasons Western Medicine so misunderstands magnesium deficiency is how they test it: with blood tests. Blood tests do not yield ANY information about magnesium. Why? Because the body controls the levels of blood magnesium very tightly. If the magnesium in the blood drops even a little bit, you’re going to have a heart attack. It’s that simple. So to prevent this, the body will rob all of its cells, tissues, and bones of magnesium in order to keep the blood levels constant. If you do a blood test for magnesium, the cells could be completely empty while your blood levels remain constant. What’s worse is that magnesium is not even in your blood. 99% of the magnesium in the body is stored in the cells that get robbed, while a mere 1% of your body’s total magnesium is in the blood. These tests are a complete waste of time, and doctors are not being educated about this reality. “A serum test for magnesium is actually worse than ineffective, because a test result that is within normal limits lends a false sense of security about the status of the mineral in the body. It also explains why doctors don’t recognize magnesium deficiency; they assume serum magnesium levels are an accurate measure of all the magnesium in the body.” – Dr. Carolyn Dean, The Magnesium Miracle Why Are We So Deficient? Here’s the short(ish) version: Number one, we’re being poisoned by our food. Number two, we’re increasingly stressed out. We’re running our engines on high to keep up with life, and it’s draining us. Stress hormone production requires high levels of magnesium, and stressful experiences lead to depletion of magnesium stores. Number three, we’re eating more sugar than ever. For every molecule of sugar we consume, our bodies use 54 molecules of magnesium to process it. Fourth, low levels in the soil and modern farming techniques deplete stores of magnesium. And lastly, magnesium is depleted by many pharmaceutical drugs and estrogen compounds such as oral contraceptives, antibiotics, cortisone, prednisone, and blood pressure medications (Drug-induced nutrient depletion handbook, Pelton, 2001). Diuretics in coffee and tea (caffeine) also raise excretion levels. Oh and by the way — flouride competes for absorption with magnesium! Nowadays, nearly everyone is magnesium deficient — no test needed. Refined/processed foods are stripped of their mineral, vitamin, and fiber content. These are anti-nutrient foods because they actually steal magnesium in order to be metabolized. When consumed, they demand that we supplement with magnesium or we are destined to break down eventually due to severe deficiency. As I said, sugar is the worst offender; every single molecule of sugar you consume drags over 50 times the amount of magnesium out of your body. Well, what if you eat a healthy diet? Processed products are not the only foods that are devoid of magnesium. In general, magnesium has been depleted from topsoil, diminishing dietary intake across the board. What’s worse, our need for magnesium has increased, thanks to the high levels of toxic exposure we come across in our daily lives (air, water, plastics, chemicals — the list goes on!). The soil is depleted of magnesium because of the pesticides that are sprayed on all conventionally grown plants and worldwide pollution that affects even the cleanest fields. Pesticides also kill those beneficial bacteria/fungi that are necessary in order for plants to convert soil nutrients into plant nutrients usable by humans. Are You a Cannabis User?Cannabis has so many positive effects in terms of treating diseases such as epilepsy, cancer, and more (read 1, 2, 3 and cureyourowncancer.org). Trust me, I’ll be the first to tell you I’m all for it — it’s a safe and effective herb with countless therapeutic benefits that the government has been hiding for years. The only way they want you using it is if they’ve patented one of its chemical compounds and can sell it to you for a profit. However, we should also look at what happens to our body on a cellular level if we use cannabis on a daily basis. Would you take parasite cleansing herbs every day for the rest of your life, or even every few days? Probably not. You’d take them when you’re sick or during a monthly cleanse, or else you’d develop some side effects from overuse. We need to remember that cannabis is a powerful herbal medicine and should be treated in this way. It turns out that using marijuana tends to deplete the body’s stores of magnesium, with the result that the person feels more anxious after coming down from the high. Of course, that doesn’t mean that it isn’t safe in moderation. It means that over time, if used consistently without proper balance via magnesium replenishment, it can and will cause magnesium deficiency. The Best Ways To Get Magnesium
Oxford Journals – Magnesium Basics: http://ckj.oxfordjournals.org/ Dr. Carolyn Dean, MD: http://drcarolyndean.com/ Source: Collective Evolution
0 Comments
 John Summerly Guest writer Believe it or not, everything you need to prevent or treat cancer is right inside your spice cabinet. More than just dried seeds, fruits, roots, barks or any other plant-based substances that add flavor to our foods, they also double as anti-cancer agents. More than 180 spice-derived compounds have been identified and scientifically explored for their health benefits. It is beyond the scope of a single article to deal with all herbs and spices that may influence the risk of cancer and tumor behavior, so we’ve highlighted 18 of the most powerful. Defeating a disease often labelled ‘incurable’ through conventional treatment typically happens through dietary strategies. A selection of spices can avert the multiplying of malignant cells in the body that gradually mature into insurmountable cancer cells. Spices like turmeric and saffron are inherent with medicinal properties that, when incorporated to our diet from an early stage strengthens our bodies against invasion of toxins, bacteria and viruses. A conscious effort has been made in the scientific community to provide information about the amount of spices needed to bring about a response and thus their physiological relevance. Although the health attributes associated with spice use may arise from their antioxidant properties, their biological effects may arise from their ability to induce changes in a number of cellular processes, including those involved with drug metabolism, cell division, apoptosis, differentiation, and immuno-competence. The complexity of understanding the biological response to spices first surfaces in the criteria used to distinguish what constitutes a culinary spice and how they differ from culinary herbs. These terms are often used interchangeably in the scientific and lay literature. The U.S. Food and Drug Administration (FDA) defines a spice as an “aromatic vegetable substance, in the whole, broken, or ground form,” whose significant function in food is “seasoning rather than nutrition” and from which “no portion of any volatile oil or other flavoring principle has been removed” (Food and Drug Administration 2007:205-208). While this is a viable definition, it does not consider the biological consequences of consuming these items and how they differ from herbs. The U.S. National Arboretum offers an alternative definition and describes spices as “flavorings (often of tropical origin) that are dried and culinary herbs that are fresh or dried leaves from plants which can be used for flavoring purposes in food preparation” (United States National Arboretum 2002). We must remember that the quantity of an item consumed does not dictate its importance. Thus, to avoid the health significance in any definition would appear flawed. Three types of biomarkers — exposure, effect, and susceptibility — are needed to evaluate the effects of spices in cancer prevention and therapy (see figure below). 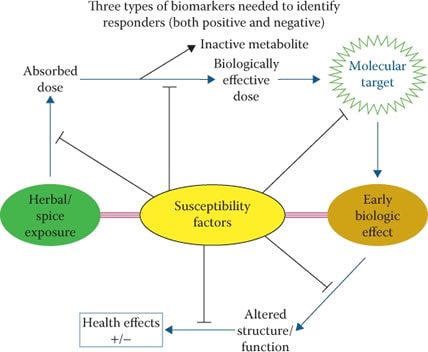 Additional information about the amounts of specific spices required to bring about a response (effect) and the interactions of spices with other constituents of the diet, microbes in the gastrointestinal tract, environmental exposures, and human genetics (susceptibility factors) will be needed to unravel the true benefits of adding spices to the diet. Spices may be a key to determining the balance between pro- and anti-cancer factors that regulate risk and tumor behavior. About 75% of households use dietary approaches to reduce their risk of diseases, including cancer. People between the ages of 36 and 55 are increasingly interested in adopting healthy eating behaviors and are gravitating toward ethnic cuisines based on perceived health benefits. Many of these ethnic foods are loaded with unique and flavorful spices; however, while dietary guidelines in several countries tend to support the incorporation of spices into diets, quantifiable recommendations for specific amounts have not yet been forthcoming. Multiple factors may influence the need for spices for reducing the risk of cancer or changing the biological behavior of cancerous cells. 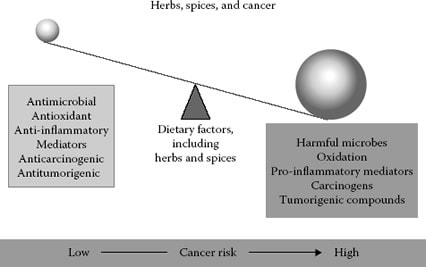 Between 1970 and 2005, the overall per capita consumption of spices in the United States doubled, increasing from about 1.6 to 3.3 pounds per year (United States Department of Agriculture Economic Research Service, 2007). As expected, the consumption of some spices increased far more than others; for example, garlic consumption increased more than sixfold. The ability of spices to serve as inhibitors of carcinogen bio-activation, decrease free radical formation, suppress cell division and promote apoptosis in cancerous cells, suppress microbial growth, and regulate inflammation and immuno-competence will be discussed as plausible mechanisms by which selected spices may promote health and disease resistance. The low toxicity and wide acceptance of spices may make them particularly useful as a subtle personal dietary change that may decrease risk for several diseases. Multiple cancer-related processes may account for the ability of spices to inhibit experimentally induced cancers. While these processes are likely critical for determining the risk of cancer and tumor behavior in humans, only limited clinical evidence exists that spices in physiological relevant exposures can alter one or more of these process. Future research should therefore focus on which process(es) is/are important for human health: DNA repair, inflammatory response, hormonal regulation, carcinogen metabolism, the cell cycle, apoptosis and differentiation. 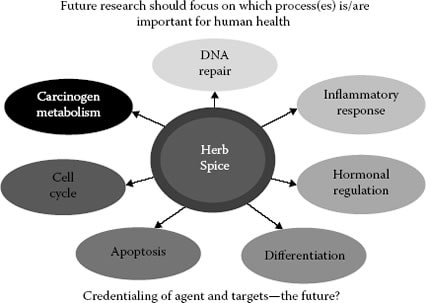  18 Powerful Spices Proven To Prevent and Treat Cancer 1. ALLSPICE The term “allspice” was coined in the 1600s by the English, who thought the herb combined the flavors of cinnamon, nutmeg, and cloves. Allspice is also referred to as “Jamaica pepper,” “kurundu,” “myrtle pepper,” “pimenta,” and “newspice.” Ground allspice is not a mixture of spices as some still believe, but arises from the dried unripe berries of the tree Pimenta dioica. This tree is native to the Greater Antilles, southern Mexico, and Central America. Today, P. dioica is cultivated in many warm areas throughout the world. Allspice is also available commercially as an essential oil. Allspice possesses antimicrobial, antioxidant, anti-inflammatory, analgesic, antipyretic, anticancer, and antitumorigenic properties (Rompelberg et al. 1996; Al-Rehaily et al. 2002; Kluth et al. 2007). It contains a multitude of potential bioactive agents that may contribute to health promotion, including flavonoids, phenolic acids, catechins, and several phenylpropanoids. The anticancer properties of allspice may be in part due to its ability to influence cytochrome P450 (CYP) activity and thereby influence carcinogen bioactivation. Kluth et al. (2007) cultured human liver carcinoma cells and human colon adenocarcinoma cells and studied the ability of the spice extract to activate mechanisms related to detoxification enzymes.  2. BASIL Basil (Ocimum basilicum) is a culinary herb prominently featured in Italian and Southeast Asian cuisines. While many varieties of basil exist, sweet basil is one of the most predominant and most frequently examined herbs for its health benefits. Basil is originally native to Iran, India, and other tropical regions of Asia, but now it is widely available throughout the world. Basil’s antioxidant, antimutagenic, antitumorigenic, antiviral, and antibacterial properties likely arise from a variety of components including linalool, 1,8-cineole, estragole, and eugenol (Muller et al. 1994; Chiang et al. 2005; Makri and Kintzios 2007). There is evidence that basil can decrease induced carcinogenesis. Providing Swiss mice with a diet containing 150 or 300 mg/kg body weight of basil extract decreased DMBA-induced skin tumors (12.5% reduction and 18.75% reduction for lower and higher doses, respectively), and lowered the tumor burden per mouse. Compared to the average number of tumors per mouse in the controls, the tumor burden was approximately 2.4 times lower in the low-dose basil group and 4.6 times lower in the high-dose basil group (Dasgupta, Rao, and Yadava 2004). The anticancer properties of basil may also relate to its ability to influence viral infections. Individuals with hepatitis B are recognized to be at increased risk for hepatocellular carcinoma (Fung, Lai, and Yuen 2009; Ishikawa 2010). Chiang et al. (2005) evaluated the antiviral activities of basil extract and selected basil constituents in a human skin basal cell carcinoma cell line against several viruses, including hepatitis B.  3. CARAWAY Caraway (Carum carvi), also known as “meridian fennel” or “Persian cumin,” is native to western Asia, Europe, and northern Africa. Recently, Kapoor et al. (2010) showed that caraway essential oil and oleoresins were progressively effectively with dose as antioxidants and more effective than commercial butylated hydroxyanisole and butylated hydroxytoluene. Schwaireb (1993) examined dietary caraway oil for its effects on skin tumors induced by DMBA and croton oil in female mice. The number of carcinomas in those animals provided with caraway oil were significantly less than in the controls. Caraway may also influence carcinogen activation by its ability to modify carcinogen bioactivation. Overall, changes in both phase I and II enzymes are consistent with the ability of caraway and its active constituent to lower chemically induced cancers.  4. CARDAMOM Cardamom refers to herbs within the Elettaria (green) and Amomum (black) genera of the ginger family. Cardamom is a common ingredient used in Indian cooking and in various parts of Europe. As with many spices, cardamom has been demonstrated to have antioxidant properties. Kikuzaki, Kawai, and Nakatani (2001) examined extracts from black cardamom (Amomum subulatum) for their ability to scavenge radicals. The ability of cardamom to inhibit chemical carcinogenesis was shown by Banerjee et al. (1994), whose observations suggest that intake of cardamom oil affects the enzymes associated with xenobiotic metabolism and may therefore have benefits as a deterrent to cancer. Cardamom has also been demonstrated to decrease azoxymethane-induced colon carcinogenesis by virtue of its anti-inflammatory, antiproliferative, and proapoptotic activities.  5. CAYENNE PEPPER The cayenne pepper — also known as the Guinea spice, cow-horn pepper, aleva, bird pepper, or, especially in its powdered form, red pepper — is a hot chili pepper used to flavour dishes. It is red colored when ripened to maturity, but also eaten while still green. It is a cultivar of Capsicum annuum related to bell peppers, jalapenos, paprika and others. Besides published evidence suggesting that cayenne pepper may aid weight loss, curb appetite, and lower blood pressure, the component that gives jalapeno peppers their heat may also kill cancer cells. Initial experiments in cancer cells and mice show that capsaicin causes prostate cancer cells to undergo a kind of suicide. Capsaicin caused almost 80 percent of prostate cancer cells in the mice to die. In addition, prostate cancer tumors treated with capsaicin were about one-fifth the size of tumors in untreated mice. Researchers speculate that, in the future, pills containing capsaicin might be used as therapy to prevent prostate cancer’s return. “Capsaicin inhibits the growth of human prostate cancer cell in Petri dishes and mice,” said lead researcher Dr. H. Phillip Koeffler, director of hematology and oncology at Cedars-Sinai Medical Center and a professor of medicine at the University of California, Los Angeles. (Their report appeared in the March 15 2006 issue of Cancer Research.)  6. CINNAMON Cinnamon is a spice obtained from the bark of an evergreen tree belonging to the Lauraceae family. Major constituents in cinnamon include cinnamaldehyde, eugenol, terpinene, α-pinene, carvacrol, linalool, safrole, benzyl benzoate, and coumarin. It takes not more than a half teaspoon of cinnamon powder every day to keep cancer risk away. A natural food preservative, cinnamon is a source of iron and calcium. Useful in reducing tumour growth, it blocks the formation of new vessels in the human body. The ability of cinnamon extracts to suppress the in vitro growth of H. pylori, a recognized risk factor for gastric cancer, gastric mucosa-associated lymphoid tissue lymphoma, and pancreatic cancer, has stirred considerable interest in the potential use of this spice to suppress human cancers (Farinha and Gascoyne 2005; Eslick 2006). Providing rats with cinnamon bark powder significantly increased several antioxidant-related enzymes in both liver and heart tissue, compared to controls (Dhuley 1999). These enzymes help maintain cellular integrity and protection against oxidative damage from free radicals.  7. CLOVE Clove is derived from flower buds of the Eugenia caryophyllata tree. Several bioactive components are found in clove, including tannins, terpenoids, eugenol, and acetyleugenol. Cloves are native to Indonesia and are used in cuisines throughout the world. While no studies have been conducted in humans to date to evaluate use of cloves in cancer prevention, a few studies conducted in mice suggest its effectiveness, especially in modifying cellular detoxification processes. Similar to allspice, clove contains high amounts of eugenol. However, this compound cannot serve to increase gastrointestinal promoter activity, suggesting other compounds in clove may account for its biological activity (Kluth et al. 2007). Overall, the findings to date suggest that tissues adapt to exposures to one or more constituents in cloves. In doing so, clove may improve the ability of selected tissues to handle foreign compounds that might lead to the initiation of carcinogenesis. Based on findings to date, additional clinical studies are warranted to determine the ability of clove to influence drug detoxification pathways.  8. CORIANDER Coriander (Coriandrum sativum) is an herb in the family Apiaceae and is native to southern Europe and northern Africa to southwestern Asia. Although all parts of the plant are edible, its fresh leaves and dried seeds are most frequently used in cooking. Coriander is a common ingredient in many foods throughout the world. One of its principal constituents is linalool. Several animal studies provide evidence that coriander seeds can promote the hepatic antioxidant system. Coriander can also influence foreign compound metabolism. Feeding Swiss mice with 160-mg coriander seeds per gram diet resulted in (glutathione S-transferase)GST induction ranging from 20% to 37%, depending on the tissue examined. In another study, Banerjee et al. (1994) observed roughly a doubling in GST activity in Swiss albino mice that were provided with diets containing coriander oil.  9. CUMIN Cumin (Cuminum cyminum) is a flowering plant in the family Apiaceae and is native to the eastern Mediterranean region and India. Thymoquinone (TQ) is the most abundant component of black cumin seed oil. TQ has been reported to exhibit antioxidant, antimicrobial, anti-inflammatory, and chemopreventive properties (Allahghadri et al. 2010; Nader, el-Agamy, and Suddek 2010). Thymoquinone that checks proliferation of cells responsible for prostate cancer. Considerable evidence also points to the ability of TQ to suppress tumor cell proliferation, including colorectal carcinoma, breast adenocarcinoma, osteosarcoma, ovarian carcinoma, myeloblastic leukemia, and pancreatic carcinoma (Gali-Muhtasib, Roessner, and Schneider-Stock 2006). The multitude of effects caused by cumin serves as justification for its continued examination as a spice with widespread potential for health promotion.  10. DILL Dill (Anethum graveolens) is a relatively short-lived perennial spice. Dill is an herb that in effect has two components that are dependent on the seasons. In the early spring, dill is used for its leaves and in the autumn for its seeds. As with other spices, there is evidence that dill promotes drug detoxification mechanisms. Because dill helps maintain cellular oxidation-reduction balance and protects cells against free-radical species, the combination of increased antioxidant levels may be particularly helpful in detoxifying foreign compounds, including carcinogens (Zheng, Kenney, and Lam 1992).  11. FENNEL Fennel (Foeniculum vulgare) is a plant species in the genus Foeniculum (treated as the sole species in the genus by most botanists). It is a member of the family Apiaceae (formerly the Umbelliferae). It is a hardy, perennial, umbelliferous herb, with yellow flowers and feathery leaves. It is indigenous to the shores of the Mediterranean but has become widely naturalized in many parts of the world, especially on dry soils near the sea-coast and on riverbanks. Fennel contains anethole, which can explain some of its medical effects: It, or its polymers, act as phytoestrogens. Armed with phyto-nutrients and antioxidants, cancer cells have nothing but to accept defeat when the spice is fennel. Anethole resists and restricts the adhesive and invasive activities of cancer cells. It suppresses the enzymatic regulated activities behind cancer cell multiplication.  12. GARLIC Garlic (Allium sativum) is a member of the onion family Alliaceae. Garlic has been used throughout history for both its culinary and medicinal properties. Garlic’s distinctive characteristics arise from sulfur, which constitutes almost 1% of its dry weight. Although garlic does not typically serve as a major source of essential nutrients, it may contribute to several dietary factors with potential health benefits, including the presence of oligosaccharides, arginine-rich proteins and, depending on soil and growing conditions, selenium and flavonoids. Preclinical models provide rather compelling evidence that garlic and its associated components can lower the incidence of breast, colon, skin, uterine, esophagus, and lung cancers. uppression of nitrosamine formation continues to surface as one of the most likely mechanisms by which garlic retards cancer. The ability of garlic to inhibit tumors due to different cancer-inducing agents and in different tissues indicates that a generalized cellular event is likely responsible for the change in tumor incidence and that the response is highly dependent on environmental or other types of biological insults. Because metabolic activation is required for many of these carcinogens, there is likelihood that either phase I or II enzymes are altered. A breakdown of allicin appears to be necessary for achieving maximum tumor inhibition. Allyl sulfur compounds preferentially suppress neoplastic over non-neoplastic cells (Sakamoto, Lawson, and Milner 1997). It is becoming increasingly clear that the response to allyl sulfurs relates to their ability to form free radicals rather than to serve as an antioxidant (Antosiewicz et al. 2008). Allyl sulfurs may bring about changes by influencing the genomic expression by affecting histone homeostasis.  13. GINGER Ginger (Zingiber officinale) is a member of the Zingiberaceae family and is consumed widely not only as a spice but also as a medicinal agent. Various animal models have been used to examine the role of ginger in cancer prevention. For example, Ihlaseh et al. (2006) exposed male Wistar rats to tumors resembling human low-grade papillary urothelial neoplasia. Rats fed with a basal diet supplemented with 1% ginger extract for 26 weeks had significantly fewer urothelial lesions compared to the controls or those fed with the diet with 0.5% ginger. Ginger also appears to have antitumorigenic properties. Several cell lines have been examined for their sensitivity to ginger. For example, alcoholic extracts of ginger inhibited tumor cell growth for Dalton’s lymphocytic ascites tumor cells and human lymphocytes. Overall, while the anticancer findings of ginger are intriguing and several processes may be associated with the observed responses, additional studies are needed to clarify the underlying mechanisms and to determine overall benefits to humans (Pan et al. 2008).  14. OREGANO Oregano scientifically named Origanum vulgare by Carolus Linnaeus, is a common species of Origanum, a genus of the mint family (Lamiaceae). It is native to warm-temperate western and southwestern Eurasia and the Mediterranean region. Oregano is high in antioxidant activity, due to a high content of phenolic acids and flavonoids. In test-tube studies, it also has shown antimicrobial activity against strains of the food-borne pathogen Listeria monocytogenes. Oregano confirms its worth as a potential agent against prostate cancer. Consisting of anti-microbial compounds, just one teaspoon of oregano has the power of two cups of red grapes! Phyto-chemical ‘Quercetin’ present in oregano restricts growth of malignant cells in the body and acts like a drug against cancer-centric diseases.  15. ROSEMARY Rosemary (Rosmarinus officinalis) is a woody herb with fragrant needle-like leaves. Rosemary is native to the Mediterranean region and possesses a bitter, astringent taste and highly aromatic characteristics that complement a wide variety of foods. Rosemary is a member of the family Lamiaceae, and it contains a number of potentially biologically active compounds, including antioxidants such as carnosic acid and rosmarinic acid. Other bioactive compounds include camphor (up to 20% in dry rosemary leaves), caffeic acid, ursolic acid, betulinic acid, rosmaridiphenol, and rosmanol. Due to its high antioxidant activity, crude and refined extracts of rosemary are now widely available commercially.While the data are difficult to interpret, when rosemary is added along with other herbs to a balsamic vinegar preparation used in soups and salads, it appears to provide protection again oxidative stress in humans (Dragan et al. 2007). Considerable evidence also suggests that rosemary extracts, or its isolated components, can retard chemically induced cancers. For example, topical application of a rosemary extract has been reported to block the initiation and promotion phases of skin tumorigenesis (Huang et al. 1994). Rosemary extracts and the active compounds carnosic acid and rosmarinic acid have been found to inhibit the proliferation of various human cancer cell lines, including human, small cell lung carcinoma, human prostate carcinoma, human liver carcinoma), human chronic myeloid leukemia, human breast adenocarcinoma, human prostate adenocarcinoma, and human breast adenocarcinoma; (Yesil-Celiktas et al. 2010).  16. SAFFRON Saffron is a spice derived from the flower of the saffron crocus (Crocus sativus) plant native to Southwest Asia. It has historically been the world’s most expensive spice per unit weight. Saffron imparts a bitter taste and hay-like fragrance to food. Saffron likely contains more than 150 volatile and aroma-yielding compounds. A carotenoid, comprises >10% of dry saffron’s mass and is responsible for the rich golden-yellow hue created when saffron is added to food dishes. Picrocrocin, a bitter glucoside, is responsible for saffron’s flavor. The natural carotenoid ‘Crocetin’ is the primary cancer-fighting element that saffron contains. It not only inhibits the progression of the disease but also decreases the size of the tumour by half, guaranteeing a complete goodbye to cancer. Though it is the most expensive spice in the world for it is derived from around 250,000 flower stigmas (saffron crocus) that make just about half a kilo, a few saffron threads come loaded with benefits you won’t regret paying for. Significant information points to the ability of saffron to inhibit cancer (Abdullaev 2003). Aqueous saffron preparations have been reported to inhibit chemically induced skin carcinogenesis (Das, Chakrabarty, and Das 2004). Both changes in carcinogen bioactivation and tumor proliferation appear to occur. Saffron and crocus also have significant antitumorigenic properties. Similar to other spices, they appear to suppress cell growth in neoplastic cells to a greater extent than in normal cells (Aung et al. 2007). The ability of crocin to decrease cell viability occurs in a concentration- and time-dependent manner (Bakshi et al. 2009). The effects of tumor suppression also have an impact on the longevity of the host. A significant increase in the life span of Dalton’s lymphoma-bearing animals was found in those provided with saffron.  17. THYME Thyme is another culinary and medicinal herb. Today, common usage refers to any or all members of the plant genus Thymus, also of the Lamiaceae family. Several active agents are reported, including thymol, carvacrol, apigenin, luteolin, tannins, terpinene, and other oils. Kluth et al. (2007) examined the effects of thyme on enzyme induction in cultured human liver carcinoma cells and human colon adenocarcinoma cells. They observed a thyme extract to activate promoters via the electrophile responsive element, thus providing potential clues about the mechanism by which thymol and carvacrol may influence enzyme expression and prevent cancer. Mounting evidence suggests that cancers are not an inevitable consequence of aging but are preventable diseases. The evidence here suggests that spices may be factors in one’s diet that may lower cancer risk and affect tumor behavior. Spices have been consumed for centuries for a variety of purposes, such as flavoring agents, colorants, and preservatives, Without question, evidence exists that multiple processes, including proliferation, apoptosis, angiogenesis, and immunocompetence, can be influenced by one or more spices.  18. TURMERIC
Turmeric (Curcuma longa) is a rhizomatous herbaceous perennial plant of the ginger family, Zingiberaceae. Turmeric has been used in India for thousands of years and is a major part of Ayurvedic medicine. It was first used as a dye and then later for its medicinal properties. Its active ingredient, curcumin, inhibits inflammatory reactions, has anti-diabetic effects, reduces cholesterol among other powerful health effects. A new study led by a research team at Ludwig-Maximilians-Universitat (LMU) in Munich now shows that it can also inhibit formation of metastases. One of the most comprehensive summaries of a review of 700 turmeric studies to date was published by the respected ethnobotanist James A. Duke, Phd. He showed that turmeric appears to outperform many pharmaceuticals in its effects against several chronic, debilitating diseases, and does so with virtually no adverse side effects. This is the king of spices when it comes to dealing with cancer diseases, besides it adding a zesty colour to our food on the platter. Turmeric contains the powerful polyphenol Curcumin that has been clinically proven to retard the growth of cancer cells causing prostrate cancer, melanoma, breast cancer, brain tumour, pancreatic cancer and leukemia amongst a host of others. Curcumin promotes ‘Apoptosis’- (programmed cell death/cell suicide) that safely eliminates cancer breeding cells without posing a threat to the development of other healthy cells. In cases of conventional radiotherapy and chemotherapy, the surrounding cells too become a target in addition to the cancer cells. Therefore, the side-effects are imminent. Duke noted that in the handbook Phytochemicals: Mechanisms of Action, curcumin and/or turmeric were effective in animal models in prevention and/or treatment of colon cancer, mammary cancer, prostate cancer, murine hepato-carcinogenesis (liver cancer in rats), esophageal cancer, and oral cancer. Curcumin may be useful in the prevention of breast and prostate cancers — which are both linked to inflammation — and in reducing their metastatic potential. It could play a positive role in primary prevention — before a full-blown tumor arises — or help to avert formation of metastases. In this context the fact that the substance is well tolerated is very important, because one can safely recommend it to individuals who have an increased tumor risk. About the author: John Summerly is nutritionist, herbologist, and homeopathic practitioner. He is a leader in the natural health community and consults athletes, executives and most of all parents of children on the benefits of complementary therapies for health and prevention. You can follow John at preventdisease.com where this article first appeared. By Dr. Russell Blaylock MD 8-16-9 Dr Blaylock's List of suggestions on How to Reduce the Toxic Effects of the A/H1N1 Vaccine, is as follows: 1. Number one on the list says Dr Blaylock, is to bring a cold pack with you and place it on the site of the injection as soon as you can, as this will block the immune reaction. Once you get home, continue using a cold pack throughout the day. If you continue to have immune reactions the following day, have cold showers and continue with the cold press. 2. Take fish oil. Eicosapentaenoic acid (EPA), one of the omega 3 fatty acids found in fish oil supplements, is a potent immune suppressant. If you take high dose EPA you will be more susceptible to infections, because it is a powerful immune suppressant. However, in the case of an immune adjuvant reaction, you want to reduce it. Studies show that if you take EPA oil one hour before injecting a very powerful adjuvant called lipopolysaccharide (LPS), it would completely block the ability of the LPS to cause brain inflammation. Take a moderate dose everyday and more if needed to tame a cytokine storm. 3. <http://lpi.oregonstate.edu/f-w00/flavonoid.html>Flavonoids are third on the list, namely curcumin, quercetin, ferulic acid and ellagic acid, particularly in a mixture. The curcumin and quercetin in particular have been found to block the ability of the adjuvants to trigger a long-term immune reaction. If you take it an hour before the vaccination, it should help dampen the immune reactions says Dr Blaylock. 4. Vitamin E, the natural form that is high in gamma-E will help dampen the immune reactions and reduces several of the inflammatory cytokines. 5. An important ingredient on the list is Vitamin C at a dose of 1000 mg, taken four times a day between meals. It is a very potent anti-inflammatory and should be taken in a buffered form, not as absorbic acid, says Dr Blaylock. 6. <http://www.naturalnews.com/002156.html> Also use astaxanthin as it's an antiinflammatory. According to Dr Blaylock, fatal reactions to vaccines in aboriginal and African children occurred in those who were deficient in carotinoids, like astaxanthin. It is a good protection against the toxic effects of the vaccine. 7. Likewise, it was found that children who were deficient in zinc had a high mortality rate. Zinc is very protective against vaccine toxicity. (Do not use zinc mixed with copper however, as copper is a major trigger of free-radical generation according to Dr Blaylock). 8. Ensure you avoid all immune-stimulating supplements, such as mushroom extracts, whey protein and <http://www.betaglucan.org/>beta-glucan. 9. Take a multivitamin-mineral daily one that does not contain iron. This multivitaminmineral is to make sure your body has plenty of B vitamins and selenium. Selenium, said Dr Blaylock, is very important for fighting viral infections and it reduces the inflammatory response to vaccines. 10. Magnesium citrate/malate 500 mg of elemental magnesium two capsules, three times a day. (This was not mentioned during the show, but was posted at Dr Deagle's website, <http://www.clayandiron.com/news.jhtml?method=view&news.id=2103>ClayandIron.com). 11. What is very important is vitamin D3, which is the only 'vitamin' the body can manufacture from sunlight (UVB). It is a neural hormone, not really a vitamin says Dr Blaylock and helps if you are over-reacting immunologically by cooling down the reaction. Similarly, if you are under-reacting, it helps to boost your immune response. In addition it also protects against microorganism invasion. Black people and those in colder climates are particularly deficient, so they will almost certainly require supplementation. Dr Blaylock recommends that following vaccination it will help to keep the immune reaction under control if: i) All children get 5,000 units a day for two weeks after the vaccine and then 2,000 a units a day thereafter; ii) Adults get 20,000 units a day after the vaccine for two weeks, then 10,000 units a day thereafter; iii) And with that adults should take 500-1000 mg of calcium a day and children under the age of 12 years should take 250 mg a day, as vitamin D works more efficiently in the presence of calcium. 12. Ensure you avoid all mercury-containing seafood or any other sources of mercury, as the heavy metal is a very powerful inducer of autoimmunity, is known to make people more susceptible to viral infections and will be in H1N1 vaccines. 13. Avoid the oils that significantly suppress immunity and increase inflammation - such as corn, safflower, sunflower, soybean, canola and peanut oils. 14. Drink very concentrated white tea at least four times a day. It helps to prevent abnormal immune reactions. 15. Pop parsley and celery in a blender and drink 8 ounces of this mixture twice a day. Dr Blaylock says the parsley is very high in a flavonoid called apigenin and that celery is high in <http://www.dietaryfiberfood.com/antioxidants/flavonoid-antioxidant.php>luteolin. Both are very potent in inhibiting autoimmune diseases, particularly the apigenin. WHAT CAN I DO TO PROTECT MY HEALTH IF I TAKE A VACCINE? This is great information. I use Homeopathy prophylactically for the flu this time of year but here are some remedies and other ideas to help you reverse and fight off the toxic effects of the vaccine if you end up having to get it. If you do this and you need help weeding through Homeopathic remedies and how to take them please don't hesitate to call me at the Falling Leaf Retreat & Wellness Center 231-944-8351. I'm a certified Homeopath. http://pandemicresponseproject.com/resources.html#ifyoumustvaccinate IF YOU MUST VACCINATE... Not intended to be or substitute for proper medical advice and supervision. This information is provided for educational purposes only. Consult a professional healthcare practitioner before administering any healthcare protocol. Vaccination Prophylactic Protocol Utilizing Naturopathy and Homeopathy 1) One month before the vaccination date: Large amounts of Vitamin C. That is,1000 mill. twice daily three weeks before the date. Then double that amount two weeks before and triple the amount the week of the vaccinations including the day of and at least one month post vaccination date. 2) On the day of the vaccinations a mixture of Hypericum 1M and Ledum 1M placed in 4 ounces of water to be sipped every 2 hours. 1 sip = 1 Tablespoon. It should be taken as close to and after the injections as possible and continued for one day after; longer if soreness occurs at the site. 3) As soon as possible after the injection, preferably within minutes, have a small baggy of Redmond Clay Conditioner, (can be found on line) that is in its natural state. The natural state is when it is dry and powdery. It should be activated with a small amount of water or saliva to make a muddy paste and placed directly on the injection site. To keep it affixed, either a large bandage with tape, a plastic bag tied around it or a handkerchief should hold the mixture in place. Soon after a new application should be put in place and repeated every few hours for a minimum of 1 week. Redmond Clay is medicinal. It binds with and draws out toxins. 4) Diatomaceous Earth or Bentonite be consumed in a beverage and drunk for the next several days. 1 Tablespoon 1-3 times per day. This will bind toxins and to aid in drawing them out. 5) Mercurius sol 30 or Mercurius viv 30 administered particularly if there are any neurological effects as soon after the vaccination as possible. 6) Probiotics and prebiotics taken every day for months in advance and months after. This can be found naturally in raw milk, yogurt, real sauerkraut or in capsule or powder form, such acidophilus. 7) Thuja 200c can be used as a finishing homeopathic remedy. It should be considered a month after the last vaccines. Sulphur can also be considered depending on pathology presentation. 8) Abstinence from junk food and in it’s place, as much coconut oil, (such as Green Pasture) raw butter, raw or at least whole dairy, rare meats and plenty of water. 9) Many of these products and remedies can be stowed away in lockers and duffle bags. Even butter and coconut oil can be kept for extended periods of time in high temperatures. Homeopathic remedies must not be exposed to heat above 120 degrees as it may render them useless. Clay and Vitamin C remain fully capable after exposure to any temperature. Avoid mint, camphor, menthol, teatree oil and other aromatics to keep from antidoting the homeopathics for at least one month. 10) For mothers who worry dreadfully about their children in this setting, the following remedies are vital and are in order of importance: Causticum, Ignatia and Argentum nit (or Arg met). To be administered by a homeopath as poetency, frequency and constitution are a consideration. Additional Homeopathic Remedies 1) Nux vomica for 2 weeks.(generally for adults) 2) Thuja 30 for 3 weeks; thrice daily 3) Sulphur, Malandrinum and Thuja are known in the medical literature to offer the ability to counter serious side effects of vaccination. 4) Silica and Thuja together have been known to be effect antidotes to Vaccinosis. 5) Bovine colostrum drunk daily 6) Colloidal silver, especially if there’s an indication of autism 7) Slippery elm tincture Please note that homeopathic experience is required in order to utilize the homeopathic remedies ( written in italics). Contact a certified homeopath for direction. Sources: Liz Potter, Isaac Golden, MD, Joette Calabrese, CCH, RSHom and Dr. Ramakrishnan  By Lisa Jenkins For those of you thinking of using 23andMe to get snp data related to MTHFR mutations or ANY other genetic issues - Please note – I recently found out that 23andMe does NOT validate ANY information reported in the “raw data file” unless it is also something they use to pull one of THEIR “health reports.” When 23andMe had their test kits on sale last year, I contacted them regarding testing for snp's associated with MTHFR (for those not yet familiar with those terms, those are genetic single nucleotide polymorphisms associated with methylenetetrahydrofolate reductase, an enzyme encoded by the MTHFR genes). My question to 23andMe at its' core was pretty simple – to find out if they still include basic MTHFR snp's in their raw data file, since they are now testing on the newer V5 data chip. The run-around I got on this simple question was more than a little baffling. Yes, I totally get that ALL 23andMe products are for our own amusement only and are not intended to be used to diagnose, cure, or treat any illness. I already understand the legalities there and know also that there can occasionally be inaccuracies in any testing process. I already knew that 23andMe doesn't pull a specific “MTHFR” data report and never did. What I did NOT know was how far this company goes just to make sure we know they find MTHFR mutations to be pretty much beneath the need for inquiry altogether. In fact, after basically telling me in their first response that they have concluded (per their literature review) that it's not related to a lot of things people “think it is,” in their second response they straight told me that if MTHFR is my primary concern they couldn't recommend use of their product . . INSTEAD of simply telling me whether or not they still test for those snp's!! 23andMe has actually dropped some 700 snp's from their V5 chip that were previously tested on V4. I have NO idea what all of those snp's were – COMT, MTRR, CBS etc. and etc. . . So if you were thinking of getting the 23andMe for the raw data file to upload to Nutrahacker, LiveWello, etc. and possibly find out more about your genetic code in relation to detox, etc. you may want to go with a different product or push your health provider to test. 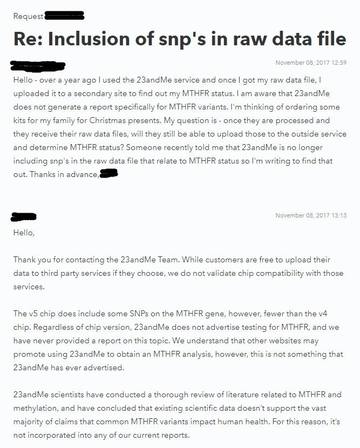 By Lisa Jenkins  RESEARCH SHOWS THAT FEWER THAN 1% OF VACCINE REACTIONS ARE BEING REPORTED:
It is well-known that VAERS (the Vaccine Adverse Event Reporting System) is a passive system and has flaws in terms of capturing the true scope of vaccine injury. VAERS was established in 1990, 28 years ago at the time of this writing. Even the CDC itself states that VAERS data is “inaccurate” in their terms. Think about it – has your doctor reported to VAERS? Do they know of the system, do they know HOW to report and what to report? Do they think that a reaction has to be SHOWN to be related to the vaccine in order to allow reporting? In fact, due to inadequate testing/tracking there is very little scientific consensus on what reactions are due to specific vaccines and reporting to VAERS is based on temporal relationship of occurrence of reactions to timing of vaccine administration. CDC's take on VAERS - “Passive surveillance systems (e.g. VAERS) are subject to multiple limitations, including underreporting, reporting of temporal associations or unconfirmed diagnoses, and lack of denominator data and unbiased comparison groups. Because of these limitations, determining causal associations between vaccines and adverse events from VAERS reports is usually not possible.” Numerous IOM (Institute of Medicine) reports going back at least 23 years have cited the failings of VAERS and have highlighted the need for more complete and accurate systems. Congressional reports on this topic have also discussed the fact that a mere fraction of the true data are indeed being reported. So is it possible that in all of that time, NO better alternatives have been explored? NOPE. Enter “Electronic Support for Public Heath - Vaccine Adverse Reporting System (ESP:VAERS)” - “The Department of Health and Human Services (HHS) gave Harvard Medical School a $1 million dollar grant to track VAERS reporting at Harvard Pilgrim Healthcare for 3 years and to create an automated reporting system which would revolutionize the VAERS reporting system- transforming it from “passive” to “active.” This project was called Electronic Support for Public Heath- Vaccine Adverse Reporting System (ESP:VAERS). According to the grant final report, the scope of the project was, “To create a generalizable system to facilitate detection and clinician reporting of vaccine adverse events, in order to improve the safety of national vaccination programs.” To accomplish this the team used the electronic medical records at Harvard Pilgrim Healthcare, Inc, which is described as a “large multi-specialty practice.” Every patient that received a vaccine was automatically identified and followed for 30 days. Within that 30 days the individual’s diagnostic health codes, lab tests, and prescriptions were evaluated to recognize any potential adverse event. Another goal of the project was to evaluate the performance of the new automated system via a randomized trial and to compare this new data to the existing data collected by VAERS and Vaccine Safety Datalink. Just the preliminary description of this program is head and shoulders above the current functioning of the passive VAERS system. In our current system, adverse events are to be spontaneously reported by parents or health care providers. Most parents aren’t even aware the VAERS system exists, much less aware that they are supposed to be reporting to it. Health care providers are “supposed” to report adverse events, but we have no idea of the efficiency level with which this is occurring, and more than a hunch that this reporting is grossly neglected for a variety of reasons. Furthermore, many vaccine adverse events are never reported because either the parent, patient, or doctor is completely unaware that a subsequent adverse event is in fact due to a vaccine. This new reporting system would remove all of these failures from the equation. NOW – After 3 years and compilation of the data, according to the published report from Harvard Pilgrim Health Care, these are the RESULTS: “Preliminary data were collected from June 2006 through October 2009 on 715,000 patients, and 1.4 million doses (of 45 different vaccines) were given to 376,452 individuals. Of these doses, 35,570 possible reactions (2.6 percent of vaccinations) were identified. This is an average of 890 possible events, an average of 1.3 events per clinician, per month. These data were presented at the 2009 AMIA conference. In addition, ESP:VAERS investigators participated on a panel to explore the perspective of clinicians, electronic health record (EHR) vendors, the pharmaceutical industry, and the FDA towards systems that use proactive, automated adverse event reporting. Adverse events from drugs and vaccines are common, but underreported. Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported. Low reporting rates preclude or slow the identification of “problem” drugs and vaccines that endanger public health. New surveillance methods for drug and vaccine adverse effects are needed. Barriers to reporting include a lack of clinician awareness, uncertainty about when and what to report, as well as the burdens of reporting: reporting is not part of clinicians’ usual workflow, takes time, and is duplicative. Proactive, spontaneous, automated adverse event reporting imbedded within EHRs and other information systems has the potential to speed the identification of problems with new drugs and more careful quantification of the risks of older drugs. Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.””* (Excerpted from the article below). WAIT A MINUTE HERE. They followed the records of these individuals for 30 days only, and identified a possible 2.6% of them that may have had a reaction to one or more of the administered vaccines in that time period?? This doesn't even get into possible effects that begin to show after 30 days (autoimmune disorders or many cancers, for example). And we're seeing 2.6% and the awareness that FEWER than 1% of possible adverse events are being reported? One would think that the CDC, if truly looking out for our best interest as consumers; would have immediately started to implement the model used by the Harvard Pilgrim group and indeed would have extended out the observation period so they could begin to determine what to study next to best refine their definitions of vaccine adverse effects and multi-vaccine effects. However, as you saw above it was quite the opposite and remains so to this day. CDC, where art thou? Allowing the recommendation of more and more vaccines on the schedule each year and utterly failing us in terms of any proper monitoring, that's where. Adding recommendations for more improperly testes vaccines for pregnant women, for infants, for the elderly, some with experimental adjuvants in them. And touting the “safe and effective” line everywhere. And HHS is right behind. Many, MANY thanks are due in helping me to write this post both to JB Handley's amazing book “How to End the Autism Epidemic” (available on Amazon) and to the following article, excerpted above and indicated with a * - http://truthsnitch.com/…/cdc-silence-million-dollar-harva…/… Read the published report from the Harvard Pilgrim Group here: https://healthit.ahrq.gov/…/r18hs017045-lazarus-final-repor… Written by Erica Dawson Once upon a time, doctors ran tests to verify whether you had a bacterial or viral infection. If your infection was bacterial, they would culture the bacteria to see which antibiotic would be most effective. Now when one goes to the doctor, they get an antibiotic no matter what issue is presenting and without verification of whether it is needed. Abuse of antibiotics has become an epidemic! Overuse of antibiotics has been a mounting concern for several years now. The prolonged and widespread overuse of antibiotics has led to the creation of many antibiotic resistant super bugs (such as MRSA, VRE, MDR-TB, and CRE, to name a few). While doctors need to be held accountable for their part in causing this epidemic, we as patients can take control of our bodies and help to end this. If your doctor attempts to give you an antibiotic "just in case", demand that they run a test to make sure that you actually NEED an antibiotic. The best way to protect yourself is to build up your immune system. Take good, bioavailable vitamins, drink plenty of water, and eat healthy! If you need an antibiotic boost, some natural alternatives are elderberry syrup (home made is best), raw or fermented garlic, or honey. Prevention is the best medicine! Overuse of antibiotics 'risks return to dark ages of life-threatening surgery' - The Guardian  We have long taught that what used to be common childhood diseases gave natural immunity to so many other illnesses and diseases. Could this be why they push the varicella vaccine so hard? History of chicken pox may reduce risk of brain cancer later in life  Just a few months ago, nobody had heard of Acute Flaccid Myelits. Now thanks to this year's #flushot, everyone knows what it is. Now they are either detracting from that or there are 2 sources. Either way, there will be a vaccine for AFM before we know it. "As the #CDC reports—with no known cause, #vaccine, or treatment— #AFM cases are continuing to grow. As of November 8th, there are now at 80 cases this year. Bennett hopes—with more known knowledge of #Levaquin—and its possible connection—medical emergencies and even death can be prevented in any medical diagnosis." Medical researchers cite possible connection to antibiotic and polio-like illness symptoms An antibiotic known by the brand name of ‘Levaquin’ is garnering national attention by medical researchers and doctors.  |
Author
Articles are written by a variety of contributors. Archives
January 2019
Categories
All
|
 RSS Feed
RSS Feed
Services |
Company |
|